an initiative by SEEK Development
Insight
0 min read
Generation Equality?

Written by
Kalila Jaeger, Zoe Johnson
Published on
March 1, 2021
Download a PDF of this Publication.
Watch a recording of the Donor Tracker webinar featuring the Kaiser Family Foundation on_ _donor funding for sexual and reproductive health and rights.
Of all the plans laid out in the Sustainable Development Goals (SDGs), SDG 5 ("Achieve gender equality and empower all women and girls") is one of the most ambitious. Throughout human history, half of the world’s population has been counted out, their intellectual and economic contributions disregarded, their bodies abused and commodified. Considerable progress has been made towards empowering women globally to live their lives autonomously. Since the adoption of the 1995 Beijing Platform for Action, 131 countries have enacted 274 laws and regulations in support of gender equality. More girls than ever before are in school, and maternal mortality rates have fallen by 38% globally. Still, massive challenges remain. Nowhere in the world are women born into full equality and, in many places, to be born female is to be born a second-class citizen.
We have already entered the final decade before the SDG’s 2030 deadline. However, progress on SDG 5 lags across a range of indicators, including targets to eliminate violence against women and girls and ensure universal access to sexual and reproductive health and rights (SRHR). To level the playing field between men and women globally will require a massive and focused international effort.
In 2020, in recognition of the importance of SDG 5 in the Decade of Action, the Donor Tracker added Gender Equality to our analyses of 14-major Organisation for Economic Co-operation and Development (OECD) Development Assistance Committee (DAC) donor markets, allowing users to compare donors’ commitments and disbursements to gender equality efforts. In addition, the Donor Tracker is publishing a series of three Insights pieces, which will provide readers with a more detailed analysis of three main elements, or ‘pillars’ of gender equality endeavors: namely, funding for women’s economic empowerment; efforts to end gender-based violence; and the fight for sexual and reproductive health and rights. This third piece analyzes existing research and newly released 2019 OECD data to assess how donor countries are approaching and, in many cases, falling short on efforts to promote sexual and reproductive health and rights in their global development programs.
Sexual and reproductive health and rights, or SRHR, is a critical element of gender equality. SRHR refers to several, interconnected freedoms and rights: the freedom to choose if, when, and how to reproduce; the right to access comprehensive sexual and reproductive healthcare; and the right to a safe and satisfying sex life with whichever partner or partners a person should choose.
At the 2021 Generation Equality Forum, donors and stakeholders will come together in a framework convention for gender equality, launching concrete, ambitious investments, and policies. Promoting universal access to SRHR resources must be a top priority in the commitments that emerge from the Forum. SRHR is crucial for people of all genders; the freedom to control the functions of one’s own body is a fundamental right, one without which all other types of freedoms fall away. Inadequate access to condoms can lead to the uncontrolled spread of sexually transmitted infections (STIs or STDs) including HIV, putting people of all genders at risk. For people who can become pregnant, lack of access to SRHR resources can lead to involuntary pregnancy, potentially turning young girls into mothers decades before they would have chosen this responsibility, often cutting off access to school, paid work, the chance at life with a chosen partner. This can undermine their ability to benefit from other efforts toward improving their social and economic mobility.
We still have a long way to go to achieve universal SRHR for people around the world:
- Approximately 218 million women of reproductive age in low- and middle-income countries have an unmet need for modern contraception1; that is, they do not wish to become pregnant but are not using a modern method of prevention. 49% of pregnancies in low- and middle-income countries are unintended (111 million annually).
- These 111 million unintended pregnancies result in 30 million unplanned births each year, 69 million abortions (of which 35 million are unsafe), 12 million miscarriages, and one million stillbirths.
- Every week, approximately 5,500 young women aged 15 to 24 years become infected with HIV. In ‘sub-Saharan Africa’2, adolescent girls account for five in six new infections. Women in this age range are two times more likely to be living with HIV than men of the same age.
To make matters worse, these major challenges to SRHR access have been further complicated by the COVID-19 crisis. The pandemic has strained health systems globally and undermined women’s access to SRHR services. Combined with an uptick in domestic violence, this means many women are facing crises of reproductive autonomy. Experts have been warning since the outset of the pandemic that a failure to prioritize SRHR services throughout the outbreak would have dire consequences. UNFPA predicted that 47 million women in 114 low- and middle-income countries would lose contraceptive access in the first six months of lockdowns resulting in seven million unintended pregnancies. For every three additional months of SRHR service disruptions, they estimated up to two million additional women would lose access to modern contraceptives globally, with unintended pregnancies increasing steadily throughout.
We likely won’t know the full measure of the COVID-19 pandemic’s consequences on SRHR access for several years to come, but understanding the funding landscape over the past decade can help inform future-oriented discussions and advocacy to ensure that donors continue to provide adequate support for SRHR through their official development assistance (ODA) despite the increased strain caused by COVID-19.
This ‘Insight’ draws on the latest OECD data to track ODA being spent on SRHR. It asks:
- How much ODA did donors spend on SRHR in 2019? How did funding change in the 10 years previous? Which are the top donor countries (in absolute and relative terms)?
- Which areas of SRHR receive the most funding and which donor countries are championing which aspects of SRHR in their ODA funding and policy?
- What resources are available for analyzing more granular funding data on the key elements of SRHR, including multilateral contributions?
Methodology
OECD data is the best way to comprehensively track donor funding for SRHR
The data for this analysis was drawn from the OECD’s Creditor Reporting System (CRS) database, which covers development assistance provided by the 30 Development Assistance Committee (DAC) donor countries, 20 non-DAC donor countries, and 46 multilateral donors. When reporting ODA to the OECD, donors mark their funding using sector and purpose codes that classify the issues being addressed by the projects their development assistance is channeled toward.
In accordance with the methodology used in the Partnership for Maternal, Newborn and Child Health’s 2020 report, ‘Funding for SRHR in Low- and Middle-Income Countries: Threats, Outlook, and Opportunities’, this analysis of SRHR looks at funding flowing to sector code 130: ‘Population Policies/Programmes & Reproductive Health’. This includes the following purpose codes:
- 13010: ‘Population policy and administrative management’, which marks ODA for population policies, demographic research and analysis, and reproductive health research.
- 13020: ‘Reproductive health care’, which includes disbursements used to fund the promotion of reproductive health, prenatal and postnatal care including delivery, prevention and treatment of infertility, prevention, and management of consequences of abortion, and safe motherhood activities.
- 13030: ‘Family planning’, which includes ODA toward counseling, information, education and communication (IEC) activities, delivery of contraceptives, and capacity building and training. Although not mentioned anywhere explicitly, funding for abortion services falls under this category.
- 13040: ‘STD control including HIV/AIDS’, which includes funding for all activities related to STDs and HIV/AIDS control such as testing, prevention, treatment, care information, education, and communication. Access to preventative care and treatment for HIV/AIDS is critical to ensuring safe, healthy sex lives are within reach for all.
- 13081: ‘Personnel development for population and reproductive health’, which marks funding used toward the education and training of health staff for population and reproductive health care services.
To illustrate the scale of funding to SRHR, this Insight also refers to “total health ODA”. This includes funding for sector codes 121: ‘Health, General’, 122: ‘Basic health’, 123: ‘Non-communicable diseases (NCDs)’, and 130: ‘Population Policies/Programmes & Reproductive Health’.
Following the broader analysis of overall funding for SRHR, this piece analyzes ODA to the three highest-funded purpose codes within ‘Population Policies/Programmes & Reproductive Health’: STD control including HIV/AIDS, reproductive health care, and family planning in more detail.
Be the first to know. Get the latest in development news, right in your inbox.
The Donor Tracker team and network of in-country experts help advocates drive sustainable impact with regular Policy Updates, data-driven analyses, and the most important news in the world of development.
By clicking Sign Up you're confirming that you agree with our Terms and Conditions.
an initiative by SEEK Development
Funding Trends
After a peak in 2017, ODA to SRHR appears to have declined to US$7.9 billion in 2019, driven by funding reductions from top donor United States; new US data may change the picture in the months to come
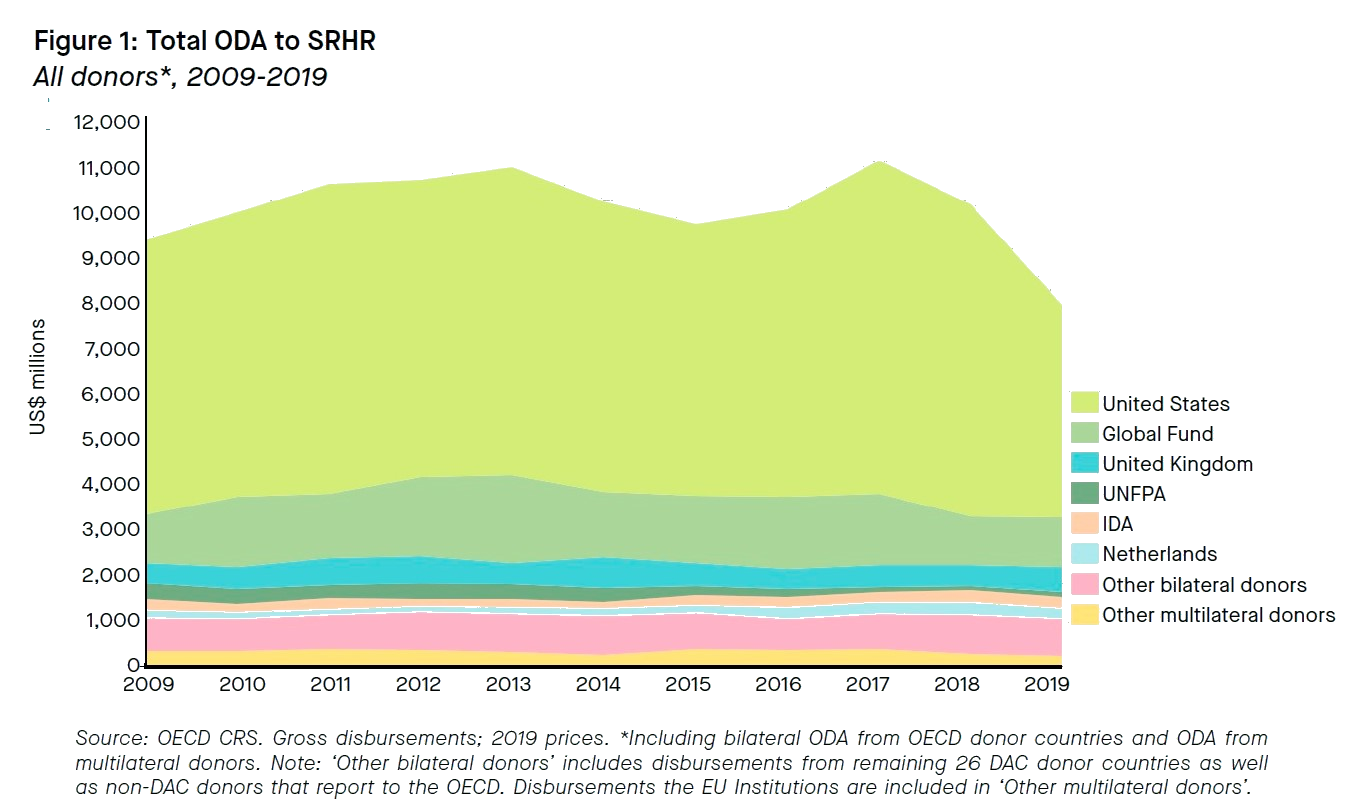
Overall, the SRHR sector saw gradual increases between 2009 (US$9.3 billion) and 2013 (US$10.9 billion), then a dip in 2014-2015 before a peak in 2017 of US$11.1 billion in total ODA (including bilateral ODA from OECD donor countries and ODA from multilateral donors). In 2019, after two years of decreases, total ODA (to SRHR was US$7.9 billion (see Figure 1). The reduction in funding since then is, in large part, attributable to what appears to be a decline in funding from the US, particularly in the STD control subsector. However, US funding to the SRHR sectors has not fallen as sharply as 2019 OECD data appears to show. The US’ 2019 totals in the CRS database are known to be low for several reasons, but primarily because disbursements (particularly to HIV projects) have not all been reported yet. New releases of CRS data in the coming months will reflect updated US totals. It is important to note that US disbursements in the SRHR sector are not reflective of political commitments. A number of factors may cause US disbursements to fluctuate over several years, but funding provided annually by US Congress for HIV projects (pictured here as STD control) and for family planning and reproductive health projects have remained stable for several years.
Bilateral ODA from donor countries accounted for 79% of total SRHR funding over the 2009-2019 period. This includes both DAC and non-DAC donors, although the latter, which are not obliged to report ODA to the OECD, represented only 0.01% of funding. Multilateral donors (including the EU Institutions) contributed the remaining 21% (see box: ‘Top multilateral donors to SRHR’ for information on the top multilateral donors to SRHR).
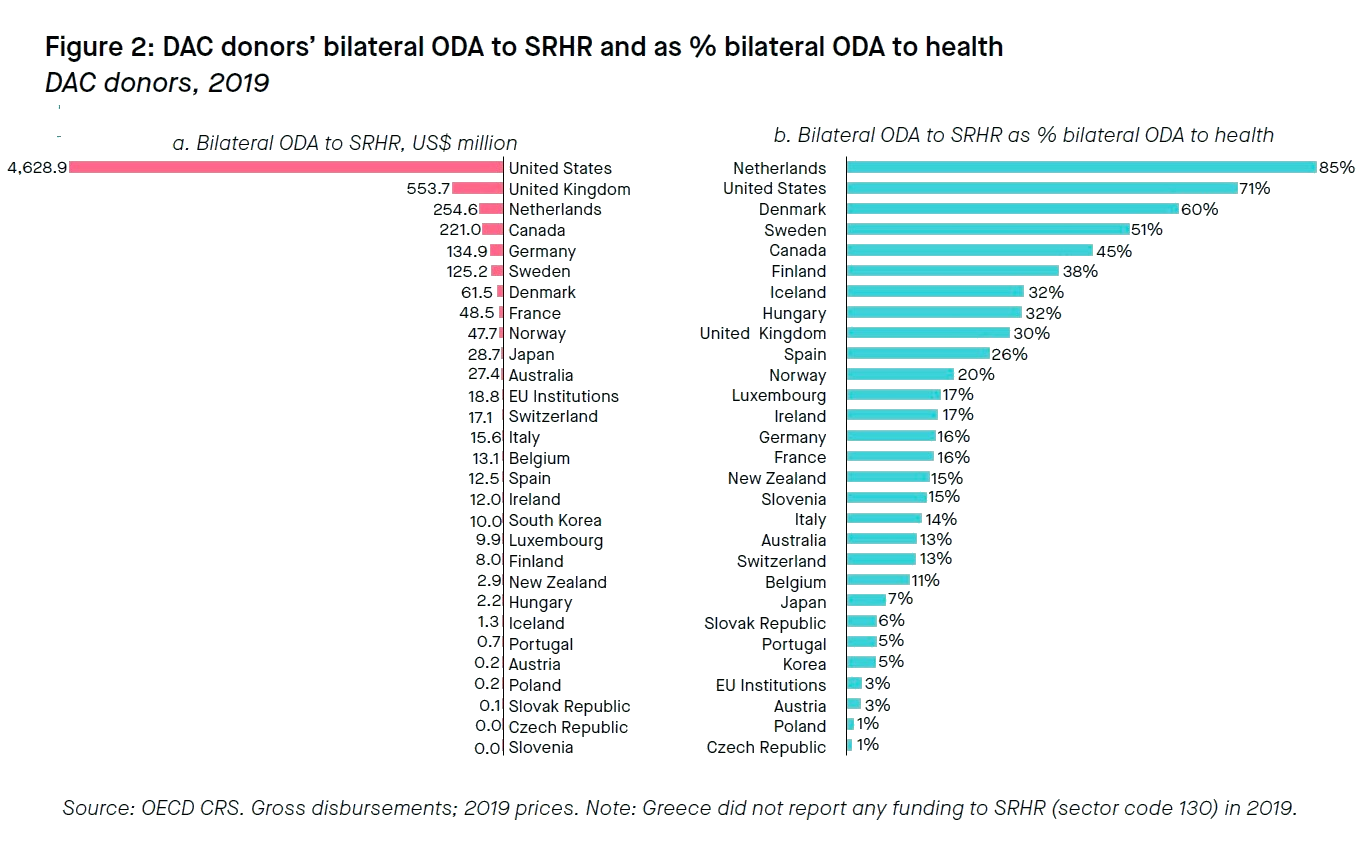
The US, the UK, and the Netherlands are the largest donor countries to SRHR; the Netherlands most strongly prioritizes SRHR in its health ODA
The US is by far the most important bilateral funder for SRHR, making up 59% of total SRHR funding (US$4.6 billion) in 2019 (see Figure 2a). Meanwhile, the UK allocated US$554 million to SRHR in 2019 and the Netherlands provided US$255 million.
The Netherlands, the US, and Denmark spent the largest shares of their total health ODA on SRHR in 2019 (see Figure 2b). In relative terms, the Netherlands topped the charts in terms of the emphasis it places on SRHR services, directing 85% of its health ODA toward SRHR projects. The US places second (71%), followed by Denmark (60%), Sweden (51%), and Canada (45%). These countries spent much more of their health ODA on SRHR than other DAC donor countries; in 2019, donor countries on average spent 23% of their global health ODA on SRHR projects.
The following section analyzes SRHR funding trends and policies of some of the most important donor countries in absolute and relative terms, namely: the US, the UK, the Netherlands, Sweden, and Canada.
For further analyses of funding for SRHR, recommended readings include:
- ‘Funding for sexual and reproductive health and rights in low- and middle-income countries: threats, outlook and opportunities’, commissioned by The Partnership for Maternal, Newborn & Child Health, which analyzes SRHR funding by both donors and low- and middle-income country governments toward SRHR between 2009 and 2017 3
- ‘Adding It Up: Investing in Sexual and Reproductive Health 2019’, a 2019 report from the Guttmacher Institute comprehensively studying the need for SRHR services in low- and middle-income countries and the impact and cost of fully funding these services
Box 1: Top mutlilateral donors to SRHR
- The Global Fund to Fight AIDS, Tuberculosis and Malaria (Global Fund): The Global Fund’s investments support access to health services for girls and women in remote communities, integrating SRHR and HIV/AIDS services with a focus on comprehensive sexual health education and the development of measures to prevent mother-to-child transmission of HIV. The Global Fund was the top multilateral contributor to SRHR between 2009 and 2019, accounting for 14% of total SRHR ODA. The Global Fund's spending in the sector peaked in 2013, when the Global Fund disbursed US$1.9 billion for SRHR, then stagnated around US$1.5 billion until 2018 when funds dropped to US$1.1 billion. The US, France, and the UK are among the top government donors to the Global Fund.
- United Nations Populations Fund (UNFPA): UNFPA was the second-largest multilateral donor to SRHR between 2009 and 2019 with 2% of total SRHR ODA. UNFPA primarily focuses on population policy, administrative management, and reproductive health. Funding to UNFPA has fallen significantly over the decade, in part due to the Trump administration's elimination of all appropriations to the Fund. In 2009, UNFPA allocated a total of US$343 million to SRHR. By 2019, the amount was down to US$113 million (core funding only; donors’ earmarked funding to UNFPA is considered ODA). The UK, Sweden, and Canada contributed the largest sums to UNFPA in 2019, including core and non-core funding.
- International Development Association (IDA): The World Bank’s IDA ranks third among multilaterals in terms of total disbursements of ODA for SRHR between 2009 and 2019, with 2% of total SRHR ODA. IDA’s funding to SRHR has held relatively steady over the last 10 years, other than a period of lower funding levels between 2012 and 2015. IDA allocated US$227 million in funding to SRHR in 2009 and US$220 million in 2019, most of which has been channeled toward STD control and reproductive health. The UK, the US, and Japan were the top donors to IDA in 2019.
Countries championing SRHR
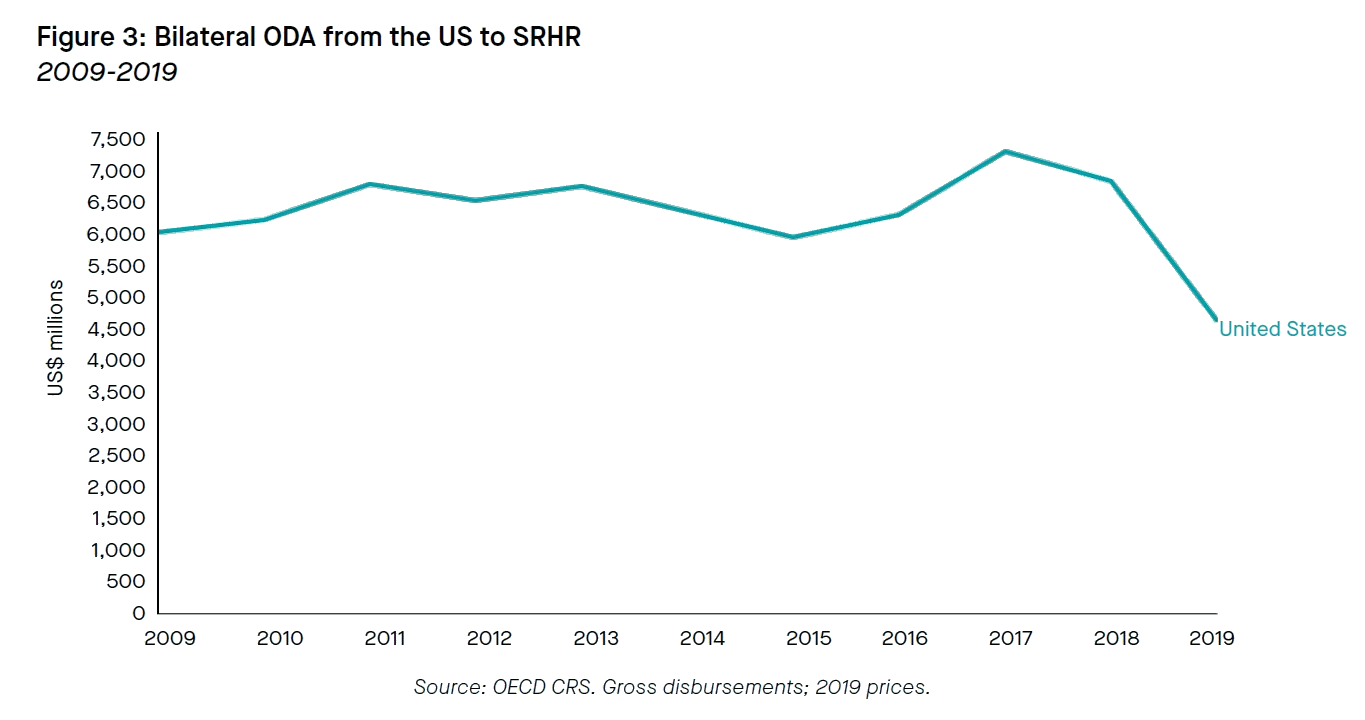
United States: the US is the top SRHR ODA provider and the volatility of American politics impacts the whole SRHR sector
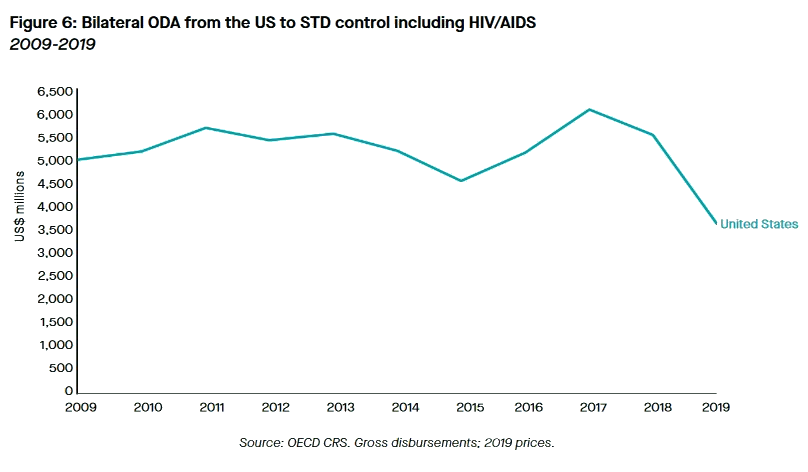
US ODA for SRHR has dwarfed funding by all other donors for at least the last 10 years. In fact, US ODA to SRHR, particularly in STD control, is on such a different scale than any other bilateral donor that a chart depicting them together is unreadable. For this reason, US funding flows to the total sector and to the STD purpose code are depicted separately from other donors (see Figures 3 and 6).
The scale of the US’ contribution to SRHR is less representative of a strong political affinity for the topic and more of the overall size of the US’ large global health budget. Because of the US’ importance for SRHR funding, US electoral politics have had an outsize impact on the landscape of the SRHR sector more broadly.4 Sex, gender, sexuality, and especially abortion are highly polarizing topics in the US. The association of these issues with SRHR funding, in particular family planning, has made ODA to SRHR a wedge issue in American electoral politics; Republican administrations repeatedly introduce policies restricting funding for family planning programs and Democratic administrations repeatedly roll back limitations to restore them. Despite political division over some types of SRHR funding, it is worth noting that US congressional support for ODA to SRHR has historically been bipartisan.
Under the Obama administration (2009-2017), the US’ ODA for SRHR increased from US$6.0 billion in 2009 to its peak of US$7.3 billion in 2017, an increase of 22%. Once in office, President Trump tried to cut US spending on SRHR initiatives across the board. Repeated attempts to slash funding to the President's Emergency Plan for AIDS Relief (PEPFAR, the US’ flagship program to combat HIV/AIDS) by US$800 million or 20% were dismissed by Congress, as were attempts to cut support for maternal, newborn, and child health (MNCH) by US$80 million. Of all SRHR subsectors, though, family planning came under the harshest, most enduring attack as the Trump administration attempted to cut US ODA to the subsector through a variety of means, only some of which were successful (see ‘Family Planning’). The reinstatement of the US’ “global gag rule”, disqualifying any organization which provides or refers out for abortion services from receiving US global health funding (see Box 2), caused a ripple effect across the sector, as other donor countries scrambled to fill the sudden need for funding to support the full spectrum of family planning services. Trump also eliminated all support for UNFPA, prompting other donor countries, particularly Norway and Sweden, to increase their spending.
Newly elected US President Biden has already rescinded the global gag rule. Biden also ordered the US’ withdrawal from the Geneva Consensus Declaration, an anti-abortion declaration signed by 34 conservative countries. So far, Biden’s first budget proposal has been significantly delayed but once published, it will provide more information about funding levels to global health projects writ large, as well as SRHR and family planning specifics, and give a better picture of Biden’s vision for the US as a provider of SRHR ODA.
Box 2: Understanding the US’ Global Gag Rule
The Mexico City Policy, also known as the ‘global gag rule’, is a US policy prohibiting international organizations from receiving US funding if they provide abortion services, referrals to the same, or advocacy for abortion law reform, even if they use other, non-US funds for those programs.
The rule was first enacted in 1984 under Republican President Ronald Reagan and since then it has been rescinded and reinstated by every administration in turn along partisan lines. It has been active for 21 of the past 36 years, significantly shaping US foreign assistance for global health. Under the ultra-conservative Trump administration, the policy became even more restrictive than under previous Republican leaders, extending beyond family planning groups to apply to child and maternal health, malaria, nutrition, and PEPFAR programs, among others, ultimately affecting an estimated US$7.3 billion in global health funding in Fiscal Year 2020 alone. By comparison, the policy under George W. Bush, the last US president to employ it, had applied to about US$600 million in total family planning funding.
A study from International Women’s Health Coalition two years into Trump’s expanded global gag concluded that the policy had had an especially devastating effect on the most vulnerable populations, disintegrating vital health services and limiting access to critical community providers.
Studies have shown that individuals seek out and get abortions, even in settings where they are restricted or banned. Unsafe abortion, which accounts for up to 13% of maternal deaths annually, is overwhelmingly concentrated in low-income countries. The cost of treating the 7 million women who are admitted each year to hospitals for major complications arising from unsafe abortion is approximately US$553 million, annually: more than half of all donors’ total expenditure on family planning in 2019.
United Kingdom: As the second-largest bilateral donor to SRHR, the UK has stepped up funding and political commitments to SRHR
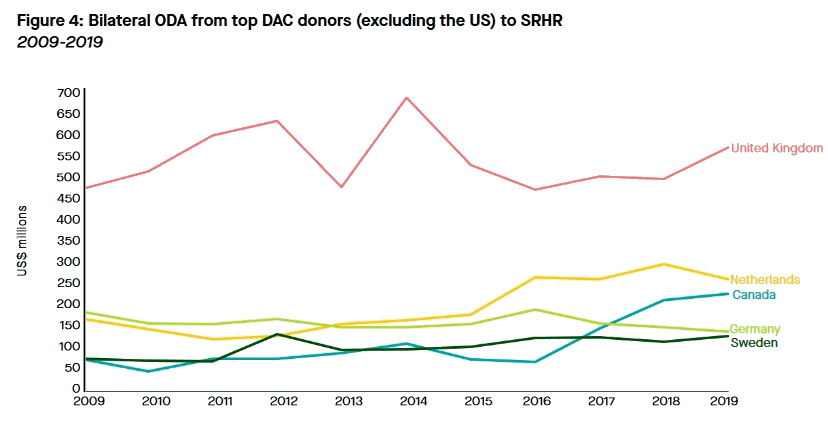
The UK’s allocations to SRHR have seen significant highs and lows over the last decade but have ultimately trended upwards from US$461 million in 2009 to US$554 million in 2019, an increase of 20% (see Figure 4).
As the second-largest bilateral donor to SRHR projects, the UK has played a major role in the international effort to maintain full-spectrum funding for SRHR as the US under the Trump administration withdrew funding from crucial pillars of the sector.
The UK’s 2018-2030 Strategic Vision for Gender Equality names "promoting universal sexual and reproductive health and rights” as one of five strategic priorities. The UK has prioritized SRHR in its COVID-19 response, by committing £10 million (US$13 million) to UNFPA’s COVID-19 response. In the spring of 2020, the UK signed a joint diplomatic statement with 59 other countries (including the Netherlands, Sweden, and Canada), vowing to protect SRHR and “promote gender responsiveness in the COVID-19 crisis”.
It is unclear whether the UK will maintain such high levels of ODA to SRHR in the years ahead. In September 2020, the UK Prime Minister merged the former Department for International Development (DFID) with the Foreign and Commonwealth Office (FCO), forming a new Foreign, Commonwealth and Development Office (FCDO). Despite reassurances from the FCDO that gender equality, including SRHR, will remain central to its mandate, the department’s failure to formally adopt the Strategic Vision for Gender Equality (introduced in 2018 by DFID) has raised concern among gender advocates.
This concern is compounded by the November 2020 announcement that the UK will only spend 0.5% of gross national income (GNI) on ODA starting in January 2021, rather than the formerly legally mandated target of 0.7%. This, combined with the fall in UK GNI as a result of the economic impact of the COVID-19 crisis, will result in a substantial decrease in volumes of UK ODA. So far, the government has not released comprehensive information about exactly which projects will be impacted by these cuts, but given the scale of the expected decreases, it is safe to assume negative implications for SRHR funding levels as well.
The Netherlands: The Dutch government has championed the global movement for women’s right to choose
The Netherlands has significantly increased ODA to SRHR over the last decade with funding starting at US$164 million in 2009, peaking in 2018 at US$289 million, and decreasing slightly again in 2019 to US$255 million: 55% more than the 2009 allocation (see Figure 4).
With ‘Sexual and reproductive health and rights’ as one of eight overarching development priorities, the Netherlands is a proven international leader on this topic, with a special focus on family planning and the rights of minorities and vulnerable populations, including sex workers and LGBTQ+ people. The Dutch Minister for Foreign Trade and International Development in 2017, Lilianne Ploumen, founded ‘She Decides’, an international organization established in response to Trump’s signing of the expanded global gag rule, which galvanizes political support for women’s social and political rights to make informed decisions around their sexuality and reproduction. In the first year following the implementation of the expanded global gag rule, ‘She Decides’ raised US$453 million in additional funds (i.e. funds not already pledged or budgeted at the time of the initial pledging conference). Sigrid Kaag, Ploumen’s successor, has continued working to keep SRHR in the spotlight of the Netherlands’ ODA policy.
With the Netherlands’ federal elections scheduled for March 2021, it remains to be seen which changes, if any, are to be made to the country’s strategy on SRHR, but the outgoing government has made an effort to reassure the public that SRHR is still a top priority. Addressing the Dutch parliament in October of 2020, Kaag reiterated that, despite a contracting economy, the government was committed to maintaining budgetary levels in its framework protecting SRHR and women's rights abroad.
Sweden: Consistently elevating SRHR on the international agenda and mainstreaming SRHR in its own global health programming, Sweden exemplifies SRHR leadership
Sweden’s funding for SRHR has steadily increased over the last ten years with disbursements starting at US$74 million in 2009, peaking in 2012 at US$129 million, and settling at US$125 million in 2019: a 74% increase over ten years (see Figure 4).
As the first country to adopt a feminist foreign policy in 2014, Sweden has long been viewed as a trailblazer in the field of gender equality generally, and particularly in the world of SRHR, which is one of six objectives of the policy framework. Funding to the sector has been increasing since the start of the decade.
Sweden lobbied aggressively for SRHR to be included in the 2019 UN Political Declaration on Universal Health Coverage and, the same year, released a new government 2019-2023 engagement strategy for the Global Fund, with a focus on promoting SRHR in health system strengthening projects.
Canada: With its Feminist International Assistance Policy, Canada has joined the ranks of SRHR champions
Canada has significantly increased funding for SRHR over the last ten years (see Figure 4). With a starting point of US$71 million in 2009, Canada scaled up its allocations starting in 2017 with US$141 million, eventually reaching US$221 million in 2019: 211% growth over ten years.
Health is a cornerstone of Canada’s Feminist International Assistance Policy (FIAP), in particular, SRHR and maternal, newborn, and child health. Canada’s development policy frames SRHR as fundamental to the empowerment of women and girls.
Canada was an active participant in global efforts to blunt the effects of the global gag rule, including through contributions to ‘She Decides’. Canada hosted the 2019 Women Deliver conference in Vancouver, where Prime Minister Trudeau announced an annual commitment worth US$1.1 billion to support women’s and girls’ health for ten years beginning in 2023, with US$540 million dedicated to SRHR annually.
The following section analyzes SRHR funding trends to the three purpose codes within SRHR that received the most ODA over the last ten years. These are STD control (including HIV/AIDS), reproductive health care, and family planning. It also includes links to further readings that provide more in-depth analyses of these issues.
Highest ODA-funded SRHR subsectors
STD control: In the last ten years, almost three quarters of SRHR ODA went to STD control, including HIV/AIDS
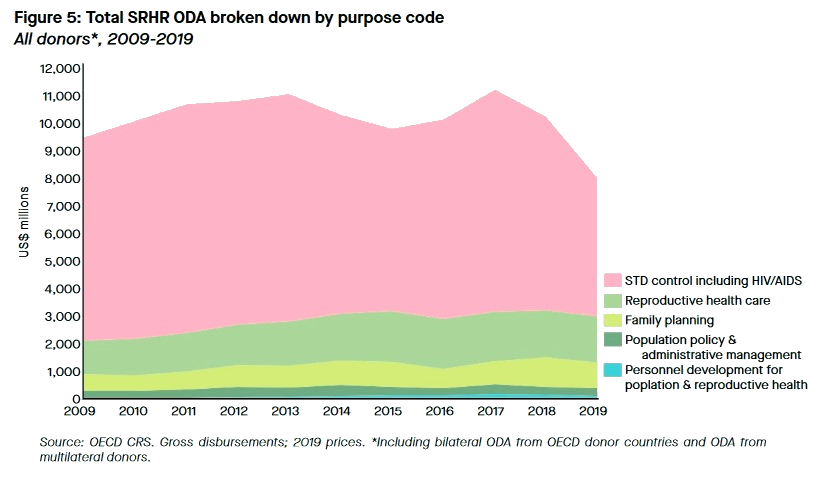
The sheer scale of the global effort to eradicate HIV/AIDS and the fact that all HIV-related projects are considered by the OECD to fall under SRHR means that STD control projects comprise the majority of the sector (see Figure 5). In 2019, total ODA for STD control stood at US$5.0 billion or 63% of total funding to SRHR that year.
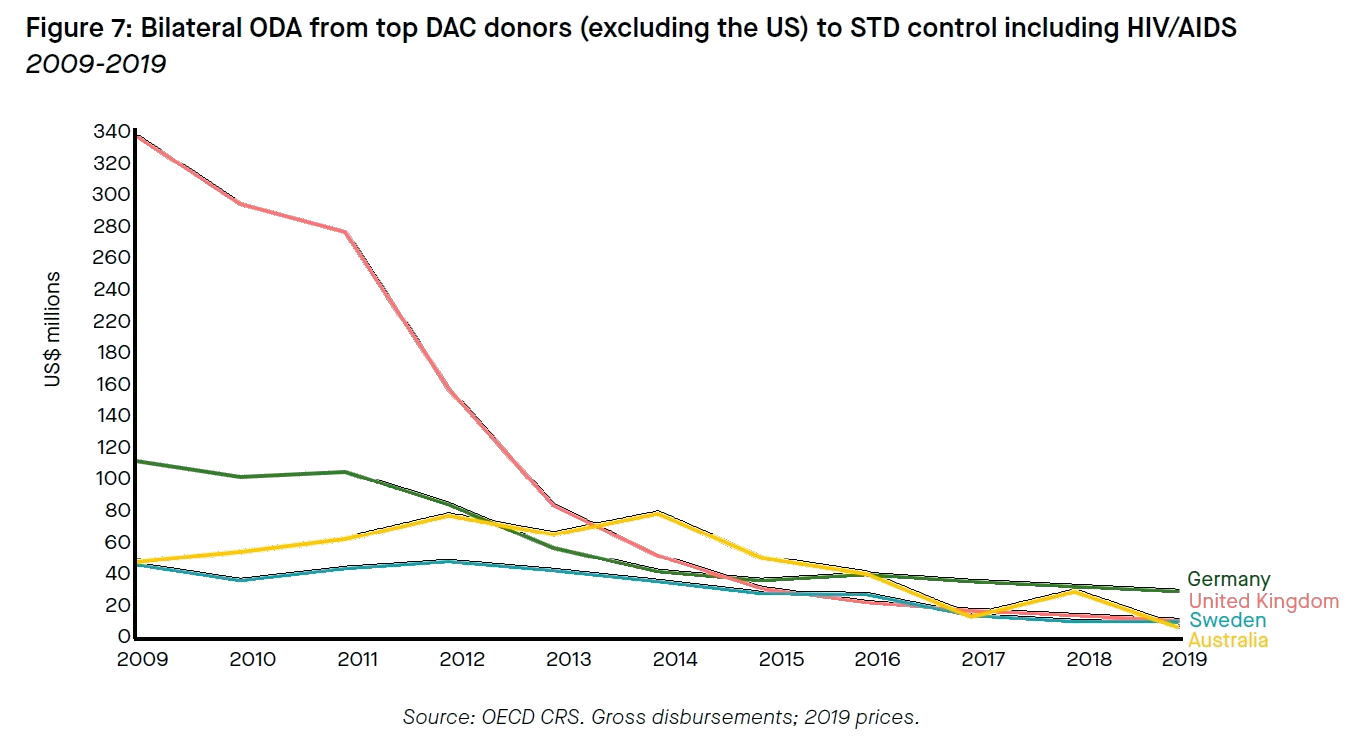
STD control still attracts the largest share of ODA for SRHR, but funding to the subsector has fallen by 36% over ten years. STD control ODA reached a peak in 2011 with a total of US$8.2 billion, of which US$5.7 billion was provided by the US. In the years following, nearly every major donor country decreased spending on STD control resulting in a loss of US$1.6 billion in over four years and culminating in a 2015 crash (see Figures 6 and 7). Stark reductions in funding, particularly from the US and UK, and a gradual withdrawal from the sector by Germany primarily powered the decrease.
The decline of ODA to the STD control purpose code is also likely a reflection of the success of global efforts to combat the spread of HIV/AIDS and to reduce the number of associated deaths. Mortality rates have fallen by 49% since 2005; however, according to UNAIDS, an additional US$26.2 billion is still needed to meet the global ‘Fast-Track’ targets by 2030.
For further analyses of funding for STD control including HIV/AIDS, recommended readings include:
- The Kaiser Family Foundation (KFF) report ‘Donor Government Funding for HIV in Low- and Middle-Income Countries in 2019’, written in collaboration with the Joint United Nations Programme on HIV/AIDS (UNAIDS), tracks spending by donor governments to HIV, relying on data collected directly from donors, from the OECD CRS, and UNAIDS records
- UNAIDS’ report, ‘UNAIDS data 2019’, which provides important context with information on progress made against the HIV epidemic as well as remaining challenges
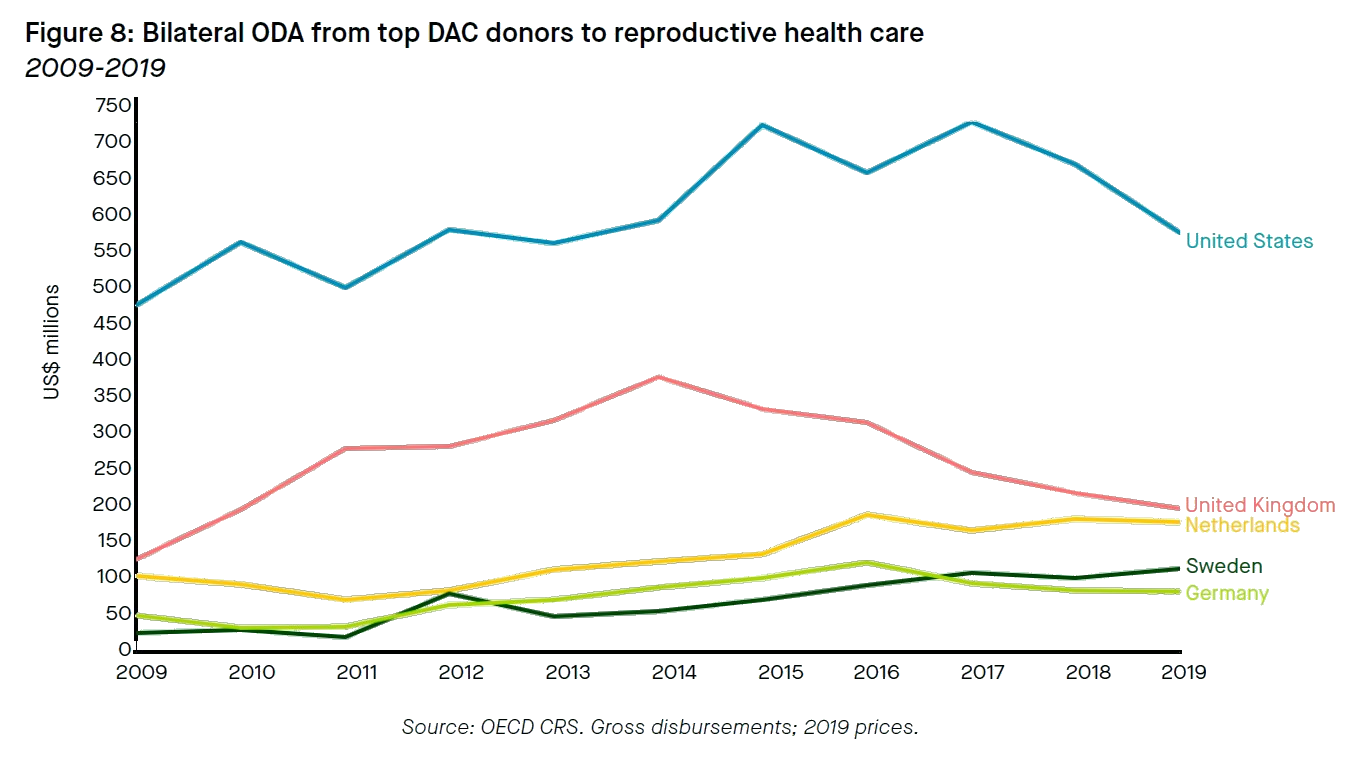
Reproductive health care: Funding for reproductive health care increased steadily until 2015, then stagnated
Reproductive health care is the second most highly funded issue within SRHR, accounting for 16% of total ODA to SRHR between 2009 and 2019 (see Figure 5). In 2019, funding for reproductive health care totaled US$1.7 billion, or 21% of SRHR funding (see Figure 8).
From 2009 to 2015, total funding to reproductive health care increased at a fairly steady rate, reaching a peak of US$1.8 billion in 2015. The largest donor countries to this subsector are the US and the UK, with the US primarily responsible for the influx of funds to the reproductive health care purpose code in the first half of the decade.5 Between 2009 and 2017, the US nearly doubled its spending to a peak of US$707 million, before delays in the disbursement of US funding resulted in a sharp drop to US$560 million in 2019.6
The UK, the second-largest bilateral funder to the purpose code, tripled its spending on reproductive health over the first half of the decade between 2009 and 2015 to reach US$368 million. The second half of the decade saw another decrease in UK spending, with funds dropping again by almost 50% down to US$192 million in 2019.
The Netherlands, the third-largest donor country to reproductive health, has gradually increased funding over the decade, from US$102 million in 2009 to US$174 million in 2019. This is consistent with an increase in Dutch spending in the SRHR sector at large over this period.
For further analyses of funding for reproductive health, recommended readings include:
- ‘Estimates of aid for reproductive, maternal, newborn, and child health: findings from application of the Muskoka method, 2002–17’ a technical Lancet paper which illustrates the complexity of SRHR funding through an analysis of ODA to reproductive, maternal, newborn, and child health across a large set of purpose codes
Family planning: with US’ global gag rule back in effect, other donor countries stepped up support for full-spectrum family planning
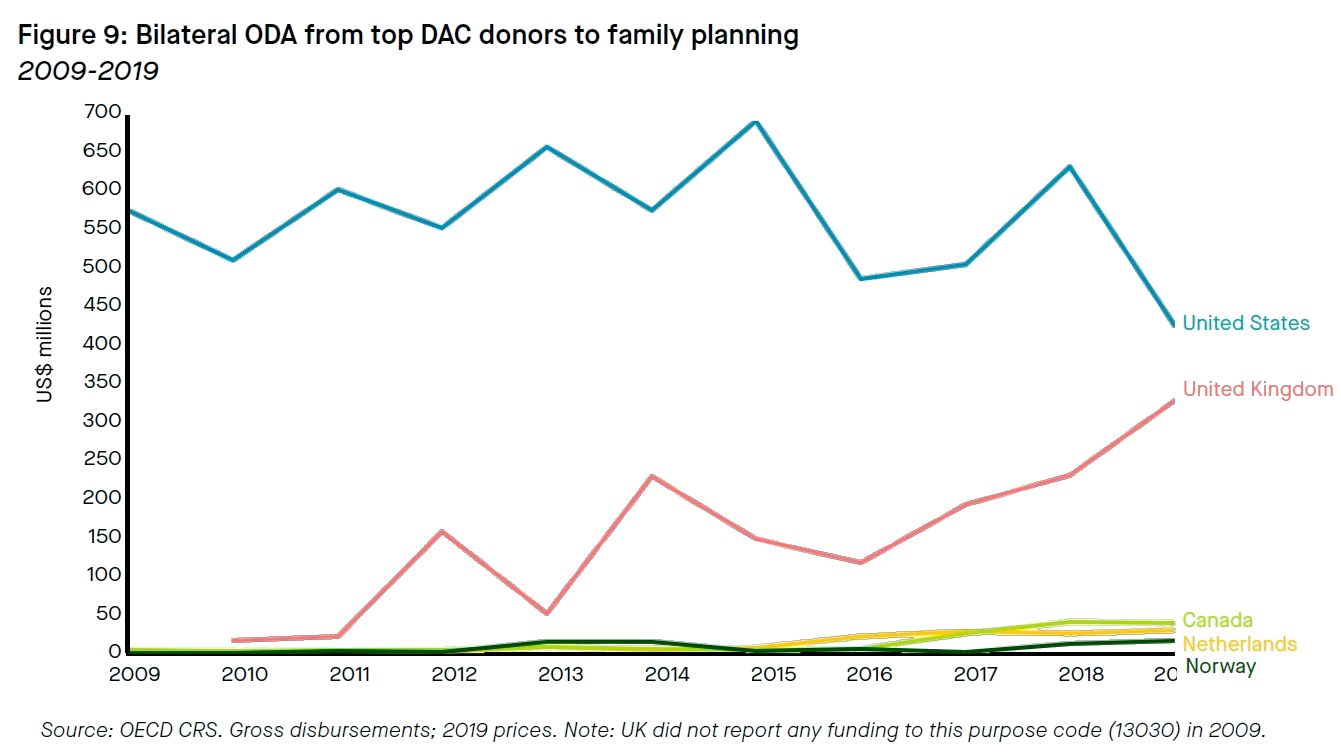
Family planning ranks third among the top-funded subsectors of SRHR and accounted for 8% of total SRHR ODA between 2009 and 2019 (see Figure 5). In 2019, family planning projects received US$930 million in ODA (bilateral and multilateral), or 12% of total ODA to SRHR. Family planning allocations have increased gradually over the decade, with the US, UK, and Canada as top donor countries.
The US was by far the largest donor to family planning between 2009 and 2019, providing 73% of the total funding to the sector throughout the decade. Although Figure 9 appears to show a marked decrease in US ODA for family planning between 2018 and 2019, this is largely due to the timing of disbursements; in fact, US bilateral appropriations for family planning remained steady during the Trump administration, despite the president's efforts to eliminate or drastically cut funds.
The reinstatement of the global gag rule in its expanded form reshaped the sector as other donors rallied together. The overall growth in funding for family planning in the years following was therefore primarily driven by increased allocations from non-US donor countries (see Figure 9), namely the UK (which nearly tripled funding levels between 2016 and 2019 to US$322 million), Canada (which increased funding to family planning nearly eight-fold between 2016 and 2019 to US$39 million) and Norway (which tripled funding in the same timespan to US$30 million).
The UK, the second-largest bilateral ODA provider to family planning in 2019, spent US$322 million for the purpose code. Starting in 2012, the UK hosted its first yearly Family Planning Summit, committing to spending an average of £180 million (US$242 million) annually until 2020. In 2017, the UK reported that it had so far supported eight and a half million women in accessing modern contraception, and committed to redoubling efforts to spend £225 million (US$301 million) yearly for five years. In a thinly veiled reference to the US’ withdrawal from the sector, the report specifically referred to providing “predictability” to “allow [partners’] long term planning”. Family Planning 2020, a global organization working with governments, civil society, multilaterals, philanthropists, and the private sector was also born out of the 2012 Summit and has since become a key player in the family planning sector.
At the 2019 UN General Assembly, the UK announced a £600 million (US$767 million) package for family planning in low-income countries, a move viewed by many as an open rebuke of the Trump administration, whose delegation at the event had called for the term “sexual and reproductive health and rights” itself to be removed entirely from UN documents. The five-year funding envelope was the UK’s largest ever standalone package for family planning and included financial support for abortion in countries where those services are legal.
Canada also significantly stepped up its commitments to the family planning purpose code in 2017 to address funding gaps caused by the US’ expanded global gag rule, raising its rank among donor countries to the third-largest in the subsector. Canada made two major pledges that year: US$15 million at the 'She Decides' conference, plus US$501 million to be disbursed over three years to fill gaps in global SRHR funding.
The Netherlands, too, has taken on a significant leadership role in the family planning subsector. Even before the US implemented the global gag rule, the Netherlands had started to scale up its funding for family planning, tripling spending between 2015 and 2016 to a total of US$21 million, ultimately reaching US$30 million in 2019. With the US abdicating its role as a global leader in the family planning space, the Netherlands decided to take a bold policy and financing stance on the issue, launching the ‘She Decides’ campaign and embedding SRHR frameworks at the highest levels of its development policies.
For further analyses of funding for family planning, recommended readings include:
- The KFF’s ‘Donor Government Funding for Family Planning in 2019’. Since the London Summit on Family Planning in 2012, KFF has been producing annual reports tracking donors’ spending toward family planning. The KFF estimates differ from those presented here due to their more complex methodology, which relies on data collected directly from donors and is only supplemented with data from the OECD.
- Data on recipient-country level expenditures from Family Planning 2020, which tracks progress toward its set of indicators on family planning service provision.
Recommendations for donors
- The downward trend in ODA to SRHR funding urgently needs to be reversed. Ensuring universal access to SRHR is a core target of SDG5, and the realization of women’s freedom to control their bodies is a prerequisite for the achievement of the other SDGs more broadly. The downward trend in OECD donors’ ODA to SRHR since 2017 is highly concerning as it could jeopardize hard-won progress in the sector. DAC donor governments should ensure SRHR funding budgets are scaled up or, at the very least, protected from further funding cuts. Donor countries like the UK, the Netherlands, Canada, and Sweden, who have increased funding levels in recent years to fill the gap left by the US’ withdrawal from the sector, should maintain these higher levels, even though US funding is likely to increase again in the next four years. More broad-based funding for SRHR will leave the sector less vulnerable to the tides of US political change.
- Donors should ensure COVID-19 response and recovery programs include SRHR as a focus area. Organizations that provide on-the-ground SRHR resources will need a surge of funding in the coming years to reconnect patient networks with services to which they’ve lost access over the last year. Following a devastating loss of access to family planning services, particularly in low- and middle-income countries, more women than ever will be in need of services connecting them with modern contraceptive methods in the coming years. The COVID-19 crisis has spurred international efforts to strengthen health systems around the globe. Donors should ensure that the health efforts they fund involve support to SRHR infrastructure.
- Advocates can capitalize on key events in 2021 and current political momentum to make the renewed case for SRHR funding. The Generation Equality Forum, taking place in Mexico at the end of March of 2021 and culminating in France in June of 2021, will be a key moment for advocates to push for increased support to the SRHR sector at large. Other important moments for SRHR advocacy over the next months include the G20 Global Health Summit in May 2021 (jointly hosted by Italy and the European Commission), the G7 Summit, hosted by the UK in June 2021, and the G20 Heads of State and Government Summit in October 2021. With the whole world bearing witness this year to the importance of multilateral cooperation in addressing momentous challenges in global health, advocates have an opportunity to use these events to elevate SRHR further on the international agenda.
Footnotes
1 Modern contraceptive methods are defined here as any of the following: permanent (female and male sterilization); long-acting reversible methods (implants and IUDs); short-acting methods (hormonal pills, injectables, male and female condoms, emergency contraceptive pills, patches, rings, diaphragms, vaginal spermicides and other supply methods); lactational amenorrhea method, which involves exclusive breast-feeding for up to six months postpartum; two fertility awareness-based methods: standard days method and two day method. Traditional methods, which are not considered modern contraceptive methods in this Insight, include periodic abstinence, withdrawal, abstinence, and breast-feeding. This definition is based on a 2019 report from the Guttmacher Institute, ‘Adding it Up: Investing in Sexual and Reproductive Health 2019’._
2 UNAIDS’ ‘sub-Saharan Africa’ designation includes Angola, Benin, Botswana, Burkina Faso, Burundi, Cameroon, Cape Verde, Central African Republic, Chad, Comoros, Congo, Côte d'Ivoire, Democratic Republic of the Congo, Equatorial Guinea, Eritrea, Eswatini, Ethiopia, Gabon, Gambia, Ghana, Guinea, Guinea-Bissau, Kenya, Lesotho, Liberia, Madagascar, Malawi, Mali, Mauritania, Mauritius, Mozambique, Namibia, Niger, Nigeria, Rwanda, Sao Tome and Principe, Senegal, Seychelles, Sierra Leone, South Africa, South, Sudan, Togo, Uganda, Tanzania, Zambia, and Zimbabwe.
3 The funding figures quoted in this report may differ slightly from that of PNCH due to changes in the US$ conversion rate. In this report, spending is quoted in US$ according to 2019 prices.
4 Figure 3 appears to show dramatic peaks and valleys in US spending for SRHR; this is due to several combined factors, primarily irregular timing in disbursements, such that spending in some years appears to look twice as low or twice as high as appropriations actually were. In some cases, allocations to the SRHR subsectors did take significant cuts: for example, STD control in 2015. Because STD control is by far the largest area of US SRHR spending, these cuts pulled the whole curve down, despite the fact that spending in the other two subsectors remained steady or increased. A granular analysis of funding trends to the individual purpose codes is given later in the piece.
5 It is worth noting, however, that because the OECD purpose codes do not directly align with the budget lines in the US’ development budget, OECD data on US ODA for reproductive health care is not reflective of the US government’s understanding of their own SRHR funding priorities. For example, US funding for projects targeting maternal, newborn, and child health (MNCH), considered its own funding line in US budget documents, is grouped together under the umbrella of ‘reproductive health’ when it is reported to the OECD. Because MNCH funding is a US development priority, it represents a significant portion of US funding marked with this purpose code.
6 US Congressional appropriations provided on a yearly basis but may be disbursed over a multiyear period. The fluctuations in disbursements that the OECD data appears to show are attributable to a variety of factors including the timing of disbursements or the realignment of programs; they are not necessarily reflective of political commitments. Congressional appropriations to most U.S. programs were relatively flat during the decade between 2009 and 2019. The reproductive health purpose code now captures maternal, newborn, and child health (MNCH) funding, but until changes were made under the Obama administration, it was recorded under the basic health purpose code. The code for some (but not all) of the MNCH funding was later reallocated to the reproductive health code, resulting in further fluctuations in the US disbursements depicted in Figure 5.


Related Publications
Feminist Foreign Policies and development finance: A primer on practical applications
Tracking funding for WEE
Women’s Economic Empowerment is in the Political Spotlight but how do you Track Donor Funding toward it?
Donor Funding for SRHR
Donor Tracker Webinar featuring the Kaiser Family Foundation:
How donors are supporting gender equality
Presented at Bond's #Funding4Dev Week
Financing, advocacy, and research to end GBV
Featuring Oxfam Canada and Promundo
Donor finance for women's economic empowerment
Be the first to know. Get the latest in development news, right in your inbox.
The Donor Tracker team and network of in-country experts help advocates drive sustainable impact with regular Policy Updates, data-driven analyses, and the most important news in the world of development.
By clicking Sign Up you're confirming that you agree with our Terms and Conditions.
an initiative by SEEK Development