an initiative by SEEK Development
Insight
0 min read
Gender equality in the health workforce

Written by
Isabela Vera, Kalila Jaeger, Laura Springmann
Published on
October 25, 2019
Creating a gender-equal health workforce is increasingly recognized as a key vehicle to achieving Universal Health Coverage (UHC). Ahead of a panel on the topic hosted by Women in Global Health at this year’s World Health Summit in Berlin, we looked at how OECD DAC donors are funding gender equality in the healthcare workforce. We assess how funding flows line up with political rhetoric on the issue, discuss challenges with data validity, and highlight what kinds of development projects will need to be funded to achieve transformative change.
By Isabela Vera, Kalila Jaeger, and Laura Springmann, SEEK Development
Introduction
The push towards Universal Health Coverage (UHC) in the global health agenda is currently facing two glaring challenges related to gender equality.
The first: gender inequality in the global health workforce. Simply put, women are the powerhouse of the world’s health workforce. Women make up 70% of all health and social care workers and contribute US$3 trillion to global health annually. Yet in countries at every income level, female health workers are overwhelmingly crowded into lower-status and lower-paid sectors and jobs and are systematically passed over for promotion, meaning leadership in the global health field has remained resolutely and disproportionately male.
The second: a major global shortage of health workers, which hampers efforts by states and multilaterals to reach UHC. It is estimated that in order to achieve UHC, one of the headline goals of Sustainable Development Goal (SDG) 3, health systems worldwide would need to recruit and retain an additional 18 million workers.
The remedies for these two problems — gender inequality in the global health workforce and the insufficient number of health workers overall — complement one another. Evidence shows that addressing gender inequality in the health workforce enables better use of talent and deployment of employees overall, reduces attrition, generally strengthens health systems, and helps pave the way to achieving UHC.
The past year saw landmark commitments to gender parity in the health workforce from states and multilaterals due, in part, to the groundbreaking work of advocacy organizations such as Women in Global Health (WGH), the host of a panel on gender equality in the workforce at this year’s World Health Summit. The G7’s Health Ministers’ Meeting declaration in May 2019 underscored the need to strengthen women’s leadership in order to bolster the health sector at large. At the UN General Assembly in September 2019, world leaders publicly committed to the Political Declaration of the High-level Meeting on Universal Health Coverage — hailed as the “most comprehensive agreement ever” on global health — which included a commitment to mainstreaming gender in UHC.
Be the first to know. Get the latest in development news, right in your inbox.
The Donor Tracker team and network of in-country experts help advocates drive sustainable impact with regular Policy Updates, data-driven analyses, and the most important news in the world of development.
By clicking Sign Up you're confirming that you agree with our Terms and Conditions.
an initiative by SEEK Development
Methodology
Using OECD DAC data, we can assess how donors are funding gender equality in the workforce
It’s encouraging to see gender equality in the health workforce being increasingly discussed in the global health agenda. But how does this rhetoric match up with health financing? (The most recently available data from the OECD is from 2017. Therefore, we can’t directly assess whether political commitments made this or last year have been reflected in actual funding flows, but we can get a sense of donors’ past commitment to the sector.)
Using OECD data on official development assistance (ODA), we can estimate donor funding for gender equality in the health workforce.
Donors use the OECD’s gender equality policy marker to record ODA that targets gender equality (see box). The OECD database also provides ‘purpose codes’, used to classify the area to which development spending is directed. We determined four purpose codes – health policy and administrative management; personnel development for population and reproductive health; medical education and training; and health personnel development – to be relevant to the health workforce, based on their detailed OECD descriptions.
We can then analyze these purpose codes in conjunction with the gender equality marker to screen for funding that specifically targets gender inequality within the health workforce.
The OECD DAC gender marker: A quick guide
The DAC gender equality policy marker records development assistance activities that target gender equality as a policy objective.
The marker has three possible scores:
- Principal: gender equality is the main objective of the project/program;
- Significant: gender equality is an important and deliberate, but not the main, objective of the project/program;
- Not targeted: project/program does not target gender equality.
This Insights piece considers all ‘Principal’ and ‘Significant’ funding to be ‘gender-focused’.
Source: OECD DAC, Handbook on the OECD-DAC Gender Equality, 2016
Funding increased in 2017...
Spending by the 30 OECD DAC members on development projects which target the healthcare workforce totaled US$1.3 billion in 2017 (see Figure 1). Of the total workforce spending, 66% (US$798 million) had a focus on gender as either a principal or significant objective of the program, the highest share ever among OECD DAC donors. This is a larger share of gender-related spending than received by the health sector overall, where only 45% of funding went to projects focused on gender (see trend line, Figure 1).
This share of gender-spending also marked an increase over 2016, when only 46% (US$543 million) of development assistance for the health workforce targeted gender. Several donors – the EU, the UK, and Japan – drove the jump, nearly doubling their spending on projects with gender equality as a significant goal.
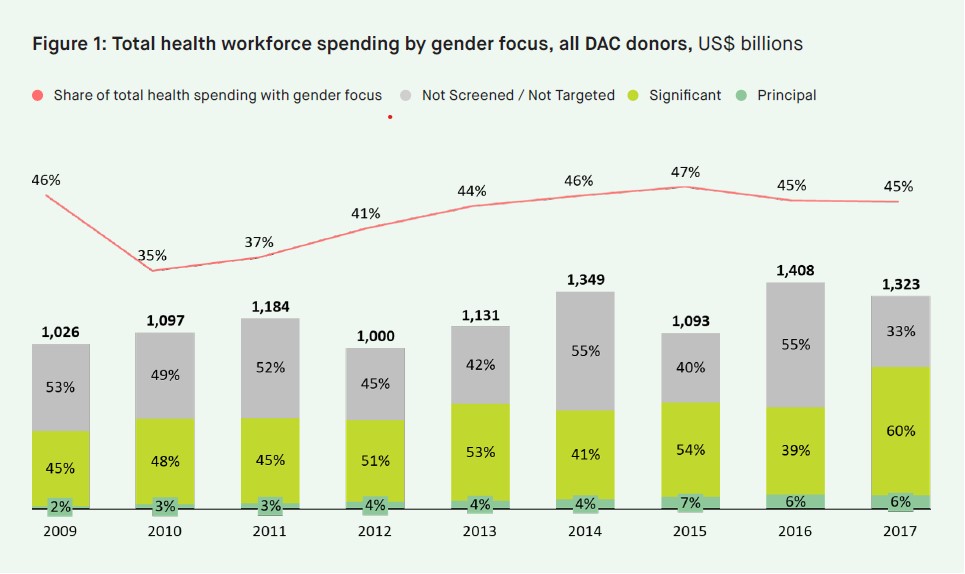
...But only 6% of health workforce-related spending primarily tackles gender inequality, and funding is stagnating
However, as a share of total workforce-related funding, we are also seeing the share of projects with gender equality as the principal goal stagnating in recent years (see Figure 1). And the share of funding for gender equality as a principal goal is woefully small compared to overall spending (just 6%, or US$83 million, in 2017). Given the importance of promoting gender equality in the workforce, these are concerning trends.
Key donors
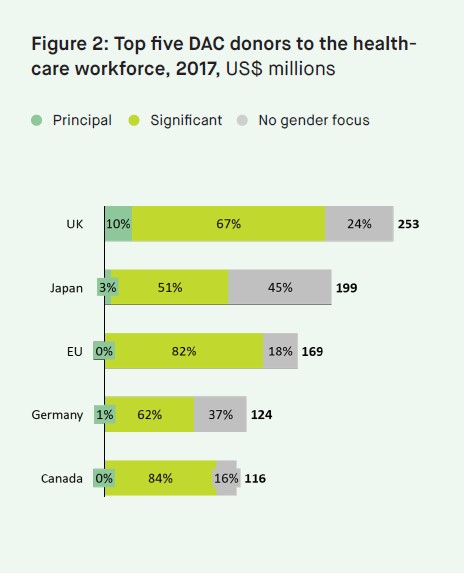
In 2017, the UK, the EU, Japan, Canada, and Germany, were the largest donors to gender equality in the health workforce. Of these donors, Canada gave the largest share of its funding to gender-related projects (84%, or US$98 million). This result is unsurprising, given Canada’s commitment to spending 80% of its development assistance on projects which integrate gender objectives by fiscal year 2021-2022 (for more on Canada’s Feminist International Assistance Policy, see our Canada Donor Profile here.) Interestingly, several top donors to global health as a whole – including the US (the largest donor) and France (the fourth-largest donor) – do not feature in this ranking. France is the 11th largest donor to the health workforce, and the US is the 20th.
Meanwhile, the UK was the only top-five donor who committed more than 3% of its funding to projects with gender equality as a principal goal – these accounted for 10%, or US$24 million) of its total spending (see Figure 2).
Focus on health policy and administration
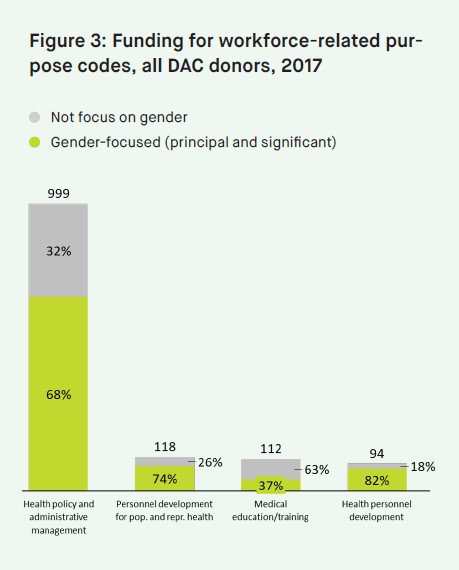
Out of our four health workforce-related ‘purpose codes’, health policy and administrative management received the most funding – nearly US$1 billion – with nearly 70% of this targeting gender equality (see Figure 3). This policy category is important: A recent working paper from WHO outlined specific labor market policy initiatives needed to counteract the gendered nature of the health workforce, including removing barriers to full-time employment for women, supporting women’s participation in higher-status areas of the health workforce, supporting gender parity in leadership positions, creating decent work conditions for all, and encouraging more research on barriers and facilitators to gender equity, particularly around mid-level, informal, and frontline health workers.
However, health policy and administrative management is a broad category. To get a better understanding of exactly what this is capturing, we did a keyword search of the OECD’s micro-dataset, which contains donor-described information on every development project reported to the OECD. Out of the 830 gender-related projects in this area, only 34 contained the word ‘workforce’, and 43 the word ‘workers’, an indication that strengthening gender equality in the health workforce is not yet explicitly a focus among donors.
Despite not finding many relevant projects in the OECD microdata set, a few top donors reported projects that seeking to catalyze policy change. Notably, ‘Employment-oriented Support to Women in the Health Sector‘, a three-year, €3 million project by Germany’s development ministry (BMZ), aims to “create a more gender-balanced health workforce in Liberia, particularly in roles traditionally dominated by men” both through policy change and by empowering women on the ground. The initiative works closely with the Liberian Ministry of Education and Ministry of Health, as well as local NGOs, to support career guidance activities, including career counseling services at secondary schools, opportunities for girls to visit high-status workplaces, and community outreach activities.
What next?
It is crucial that the increased focus on strengthening health workforces, highlighted in so many political declarations this year, translates into development projects that put gender equality in the health workforce unabashedly front and center as their principal goal. Donors should support more development projects focused on policy, advocacy, or capacity building for gender equality.
Meanwhile, health advocates should include this perspective in their efforts and highlight the ways in which proactively opposing gender discrimination improves the working conditions, efficacy, and human resource retention of the global health workforce overall.
However, to evaluate the rollout of these projects, we need better data. Given that no OECD DAC purpose code specifically captures health workforce strengthening, it is difficult to accurately track funding for the issue. This challenge could be overcome if OECD DAC donors decided to create a specific ‘purpose code’ that tracks ODA spending on health workforces.
Additionally, as we’ve noted in our recent report, ‘Words to action: The state of ODA funding for gender equality’, significant challenges remain with regards to data collection and reporting on gender equality. OECD DAC donors are marking an increasing amount of bilateral assistance as ‘unallocated’– this funding is not scored against the gender marker, making an evaluation of spending on gender equality increasingly difficult. Donors failing to screen all allocated assistance with the gender equality policy marker poses a further challenge to data precision.



Related Publications
Tracking funding for WEE
Women’s Economic Empowerment is in the Political Spotlight but how do you Track Donor Funding toward it?
Donor Funding for SRHR
Donor Tracker Webinar featuring the Kaiser Family Foundation:
How donors are supporting gender equality
Presented at Bond's #Funding4Dev Week
Financing, advocacy, and research to end GBV
Featuring Oxfam Canada and Promundo
Donor finance for women's economic empowerment
Be the first to know. Get the latest in development news, right in your inbox.
The Donor Tracker team and network of in-country experts help advocates drive sustainable impact with regular Policy Updates, data-driven analyses, and the most important news in the world of development.
By clicking Sign Up you're confirming that you agree with our Terms and Conditions.
an initiative by SEEK Development